Full-Arch Fixed Rehabilitation with Zygomatic Implants in a Case of Severe Atrophy: A Case Report by ZAGA Center Paris
Case realized by Dr. Umberto Russo, member of the ZAGA Centers network

1. Clinical Context and Treatment Limitations
The clinical course of this 46-year-old patient began with a major facial trauma during adolescence — an event that profoundly disrupted both occlusal and skeletal development.
What could have remained an isolated traumatic sequela gradually evolved, over the years, into a significant anatomical and functional disorganization. Early tooth loss, combined with prolonged use of removable partial prostheses, led to a progressive deterioration of the oro-facial balance.
The marked loss of vertical dimension resulted in severe malocclusion, joint overload responsible for pronounced temporomandibular dysfunction, and progressive mandibular decompensation. In parallel, bone atrophy — initially post-traumatic — worsened over time, reaching an extreme level in the maxilla.
By adulthood, the situation had become both anatomically critical and functionally disabling: inefficient mastication, impaired speech, and loss of occlusal stability. After several years of consultations, no conventional implant solution could be proposed, as the case’s complexity was considered beyond standard indications.
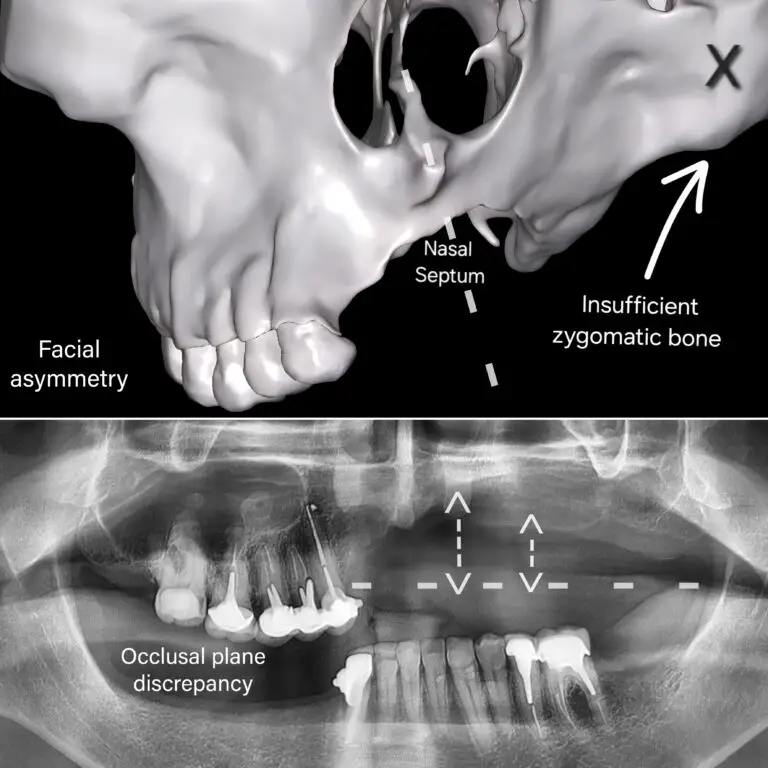
Initial Patient Condition


Clinical photographs illustrating severe aesthetic and functional impairment, and a panoramic radiograph demonstrating advanced bone deficiency.
Beyond the anatomical and functional impairments, the human impact of this condition was considerable.
The progressive deterioration of masticatory function and facial aesthetics was associated with significant psychological distress. The patient reported a near-complete withdrawal from social life, avoiding interpersonal interactions and limiting professional exchanges. The impact was such that he had gradually shifted toward exclusively remote work.
The combined functional and aesthetic impairment also compromised any normal personal projection, with a sustained negative effect on self-confidence and overall quality of life.
Despite several years of specialized consultations and repeated attempts to seek care, no surgical solution had been proposed. The anatomical complexity of the case, together with the extreme degree of bone atrophy, had led to multiple refusals, as the condition was considered beyond the scope of conventional therapeutic approaches.
2. Turning Point: Referral to a Dedicated and to Dr. Russo
Following multiple consultations with dental surgeons and implantology specialists, the conclusion was consistent: the extreme maxillary atrophy and anatomical complexity precluded any conventional implant-based solution.
In the absence of a locally available alternative, several colleagues recommended referral to a center specifically dedicated to the management of severe atrophy, where zygomatic implantology represents a reference indication.
In this context of therapeutic dead-end, the patient was ultimately referred to Sana Oris in Paris, a center recognized within the international ZAGA Centers network. The patient presented to the clinic with limited expectations, primarily seeking to understand whether any viable solution, however complex, could still be considered.
3. Radiographic Analysis and Three-Dimensional Assessment
Baseline anatomical condition: 2D and 3D imaging revealing severe bone atrophy with maxillary asymmetry.
Three-dimensional radiographic analysis revealed a particularly critical anatomical situation.
In the left maxillary sector (sector 2), residual bone was virtually absent in the posterior regions. The alveolar ridge appeared extremely thin, with insufficient height and width to support conventional implant stabilization.
In contrast, the right maxillary sector (sector 1) exhibited a distinct configuration, resulting in marked asymmetry between the maxillary halves. This asymmetry was not only volumetric but also involved the position of the sinus cavities.
The prior trauma had significantly altered the osseous architecture, leading to asymmetric sinus pneumatization with sinus floors at different levels on each side.
Residual bone density was low, and the maxillary ridge was severely resorbed. Under these conditions, not only were conventional implants contraindicated, but extensive bone grafting strategies were also considered unrealistic, given both the anatomical alterations and the limited structural capacity of the recipient site.
A comprehensive analysis of the remaining cortical structures, zygomatic morphology, and asymmetric sinus constraints was therefore performed in order to identify stable and reliable anchorage zones.
Zygomatic Arch Analysis and Therapeutic Decision-Making
Radiographic examination, however, revealed significant morphological asymmetry between the two sides.
The right zygomatic bone exhibited a relatively favorable architecture, with sufficient cortical thickness to allow reliable anchorage. In contrast, the left zygomatic bone appeared markedly thinner, with significant volumetric reduction, likely due to prior traumatic sequelae. This structural asymmetry considerably increased the complexity of implant planning.
As a result, zygomatic rehabilitation could not be approached using a standard bilateral protocol. Each side required a tailored strategy, adapted to the specific morphology and bone density of the respective zygomatic arch.
Despite these significant anatomical constraints, zygomatic implantology remained the only therapeutic option capable of providing a stable and durable fixed rehabilitation. This approach was guided by biomechanical considerations and the identification of reliable cortical anchorage, rather than by attempting an unpredictable reconstruction of an unusable maxillary bone.
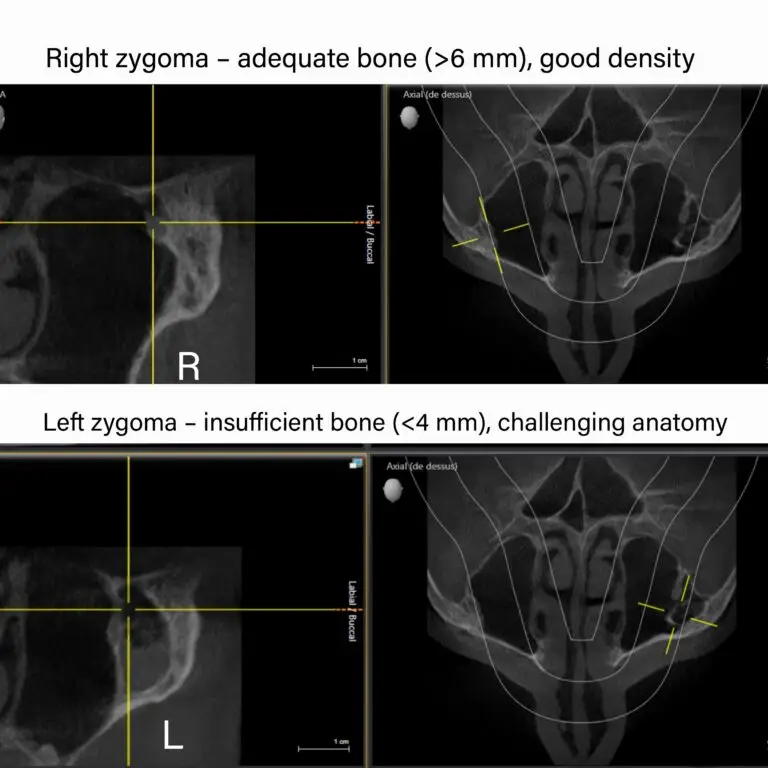
Three-dimensional analysis: coronal section demonstrating anatomical asymmetry with a significant difference in zygomatic bone volume between the two sides.
4. Surgical Procedure: Rehabilitation Using a Quad Zygoma Protocol
Given the extreme maxillary atrophy and the marked asymmetry of the osseous structures, rehabilitation was performed using a ZAGA-guided Quad Zygoma protocol, based on the placement of four zygomatic implants.
Considering the complexity of the case, the procedure was carried out under general anesthesia. A comprehensive preoperative anesthetic assessment was performed, confirming the safety conditions and validating the surgical planning.
Surgical Workflow
A custom, virtually planned osteotomy guide was designed to regularize the maxillary plane and harmonize the future prosthetic base.
Mandibular implants were placed to stabilize the lower osseous plane and re-establish a reliable occlusal reference.
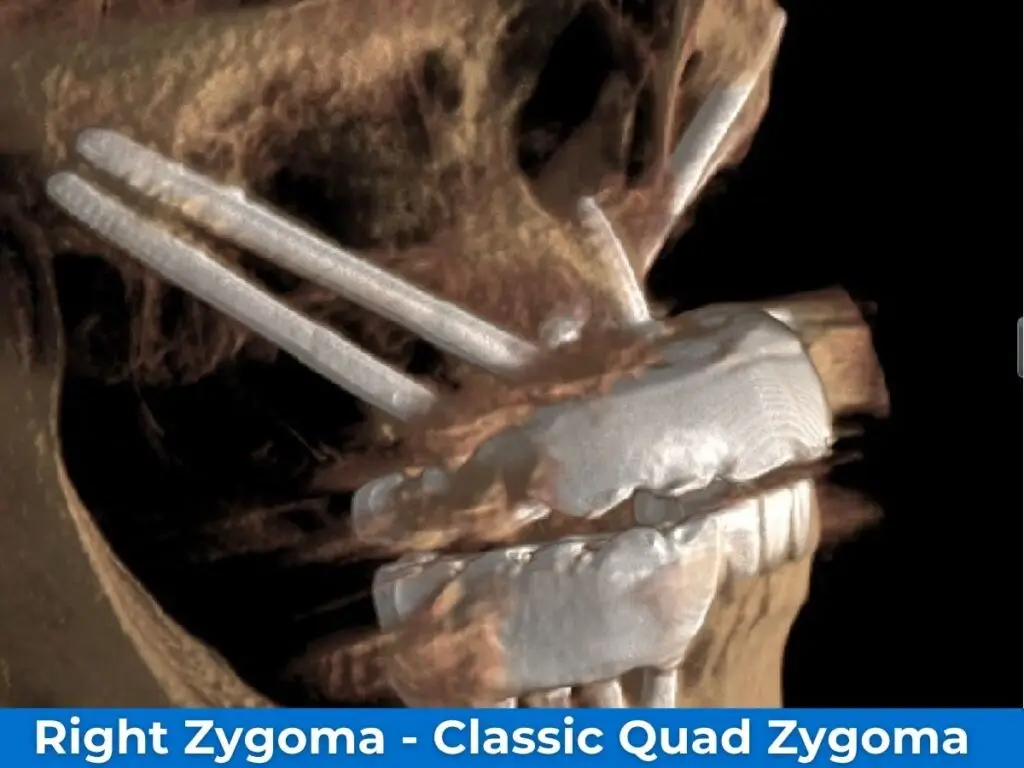
Right Side
On the right side, two zygomatic implants were placed according to the Quad Zygoma concept, a technique indicated in cases of advanced maxillary atrophy to achieve stable and secure anchorage.
Left Side
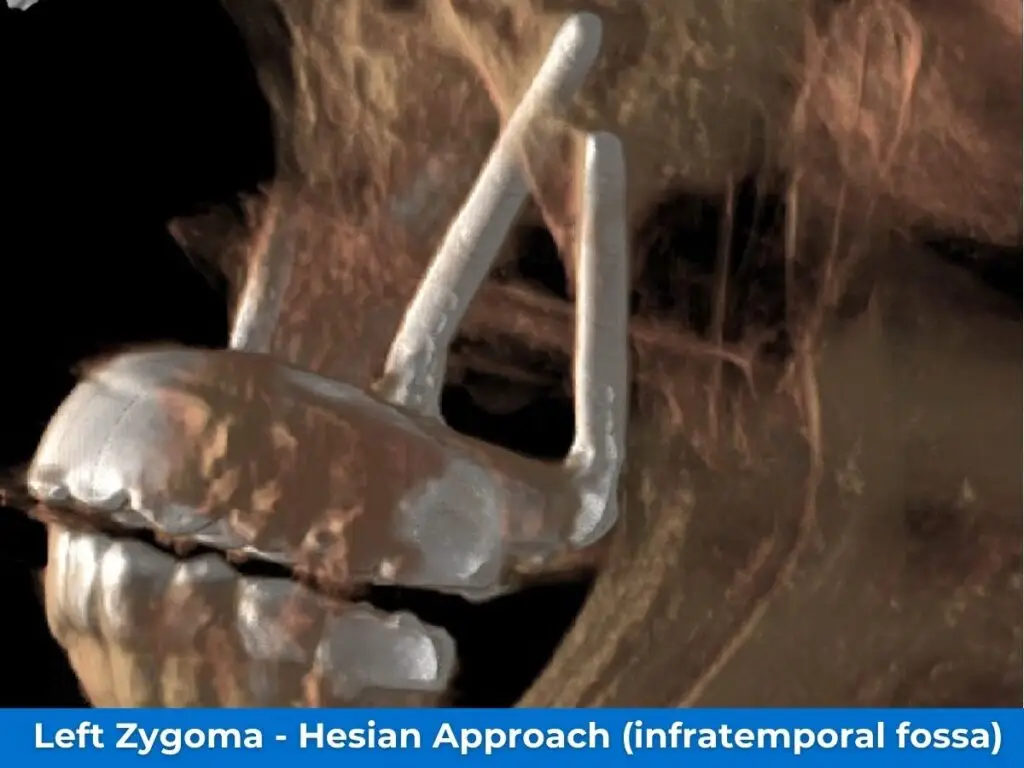
On the left side, two implants were also placed using the ZAGA approach, tailored to the patient’s anatomy and differing from the conventional Quad Zygoma protocol. The second implant was positioned posterior to the zygomatic arch, traversing the infratemporal fossa to engage a denser bone region and extend the posterior support. This configuration increased the anteroposterior (AP) spread and enhanced the stability of the future prosthesis.
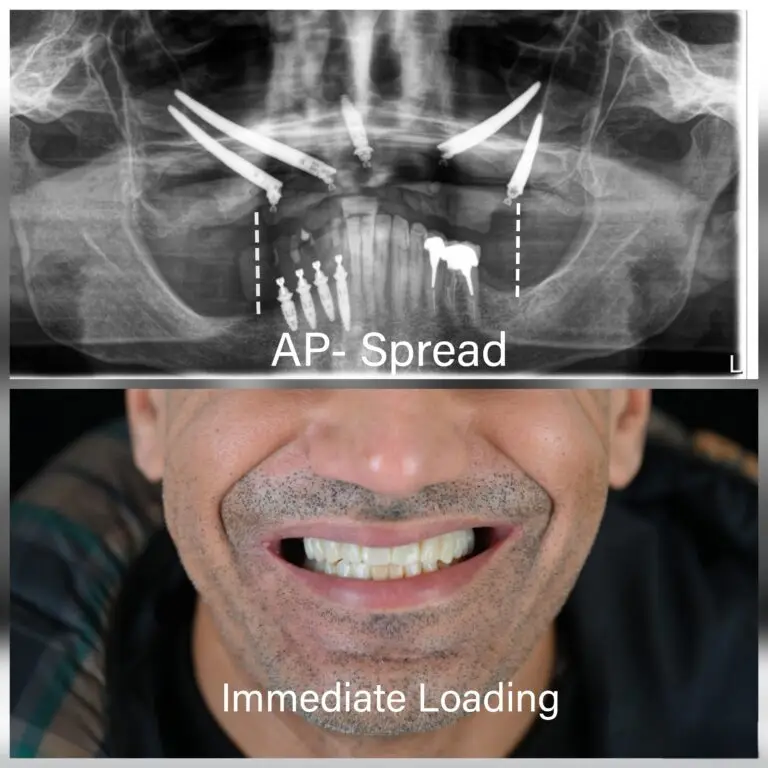
Postoperative panoramic X-ray illustrating the final implant configuration, enabling harmonious distribution of occlusal loads and reducing biomechanical stress on the future fixed prosthesis.
Optical Scan and Prosthetic Phase
At the end of the procedure, while the patient was still under general anesthesia, a three-dimensional optical impression was performed to initiate the immediate prosthetic phase. This intraoral scan, carried out by Dr. Rémy Charron, enabled precise transmission of data to the laboratory for the fabrication of the provisional fixed prosthesis. This step was an integral part of the immediate loading protocol, ensuring a rapid transition to a stable functional restoration.
5. Immediate Fixed Rehabilitation Within 24 Hours
Thanks to the primary stability achieved during surgery and the close coordination between the surgical and prosthetic teams, immediate loading was performed. In practical terms, a provisional fixed prosthesis was delivered 24 hours after the procedure.
The patient was therefore not left edentulous or with a temporary removable solution. From the day following surgery, he benefited from a complete fixed rehabilitation, adapted to the new vertical dimension and the restored occlusal balance.

In a context initially considered beyond the scope of conventional solutions, this case illustrates the potential of specialized management of extreme maxillary atrophy.
Through rigorous three-dimensional planning, precise surgical execution, and close coordination across all stages of treatment, it was possible to transform a critically compromised anatomical situation into a fully rehabilitated state within 24 hours.
At the ZAGA Center Paris, within Sana Oris, the combined expertise of Dr. Umberto Russo, Dr. Rémy Charron, and the entire team enabled the integration of advanced surgical skills, prosthetic mastery, and state-of-the-art digital technologies to deliver a stable, safe, and immediate solution.
Beyond the technical achievement, the human impact remains central. Within a very short timeframe, the patient regained effective masticatory function, a restored vertical dimension, and a level of stability that had been absent for years. Most importantly, he regained self-confidence in a situation previously perceived as irreversible.
This case represents not only a clinical success but also a highly rewarding experience for the team, highlighting that even in the most complex situations, a solution can be achieved when the treatment strategy is tailored to the patient’s specific anatomy and executed within an expert framework.
This report demonstrates that modern zygomatic implantology can transform a therapeutic dead-end into a complete functional rehabilitation, where no alternative previously seemed feasible.
6. Definitive Prosthetic Rehabilitation
After a three-month healing period, confirming satisfactory osseointegration and optimal functional and aesthetic adaptation to the provisional prosthesis, definitive prosthetic rehabilitation was performed.
This consisted of a fixed implant-supported ceramic prosthesis on a zirconia framework, designed to ensure long-term mechanical stability, optimal aesthetic integration, and full functional restoration.
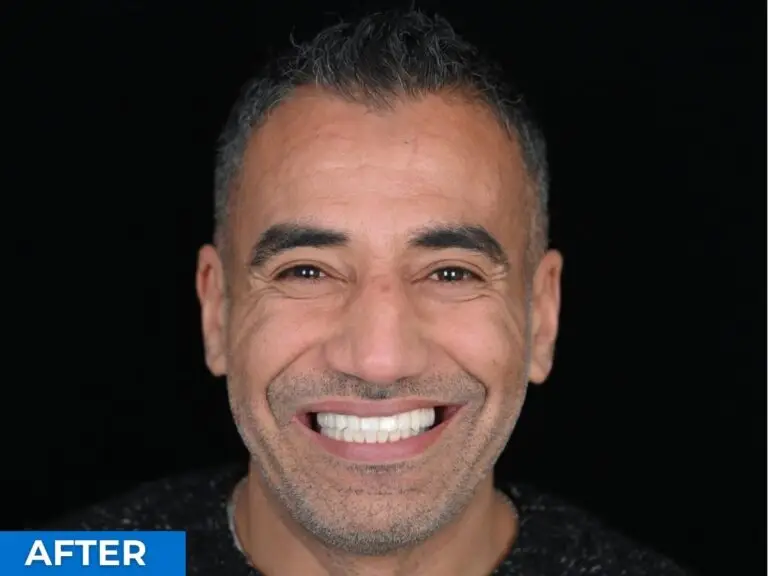
The patient fully benefited from this final outcome, with significant recovery of masticatory function and facial aesthetics, and, most notably, a marked improvement in self-confidence, reflecting a profound transformation compared to the initial condition.

Conclusion
This case highlights the complexity of extreme maxillary atrophy associated with significant anatomical asymmetry, where conventional approaches are no longer feasible. Through rigorous three-dimensional analysis, a tailored implant strategy, and rehabilitation using a Quad Zygoma protocol with immediate loading, a situation initially considered untreatable was successfully transformed into a complete fixed restoration.
When the technique is adapted to the anatomy, even the most complex cases can achieve a predictable and successful outcome.
A Special Thanks to Dr. Umberto Russo

This case report was made possible by the expertise and dedication of Dr. Umberto Russo, certified ZAGA doctor and specialist in Parodontologie e Implantologie Exclusive at ZAGA Center Paris. Dr. Russo’s mastery of the Quad Zygoma technique in this particularly challenging case — a patient previously deemed untreatable due to severe maxillary atrophy — stands as a remarkable example of what advanced zygomatic implantology can achieve.
His commitment to pushing the boundaries of implant rehabilitation has given this patient a profoundly transformed quality of life.
The ZAGA Centers network is proud to count Dr. Umberto Russo among its certified specialists, and we extend our sincere congratulations on this outstanding clinical result.