The Straumann ZAGA Zygomatic Implants
Advanced zygomatic implantS
Origins of zygomatic implants and surgical techniques

The original technique (1977)
Prof. P-I Branemark led the first developments of zygomatic implant rehabilitation. He pioneered this field by anchoring a long implant in the malar bone for the first time and allowing rehabilitation of extreme bone atrophy in the upper maxilla.
The original technique used window osteotomy on the maxillary wall to visualize the entry in the zygomatic bone. Also, the window was necessary in the pioneering phase due to the limited 3D visualization techniques at the time. Performed in combination with block bone grafting, the original technique subsequently evolved, including the following main surgical techniques:

The slot technique (2000)
The slot technique indicated a reduced window osteotomy in the shape of a slot around the implant osteotomy. Published by Stella and Warner (Stella JP, Warner MR. Sinus slot technique for simplification and improved orientation of zygomaticus dental implants: a technical note. Int J Oral Maxillofac Implants 2000 Nov-Dec;15(6):889-93), the technique reduced its invasiveness compared to the original technique.
The implant path was still intra-sinus, leading to similar potential complications as the original technique: a poor prosthetic emergence and bulky prosthesis, as well as the risk of rhinosinusitis.

The extra-maxillary technique (2006)
Dr. Carlos Aparicio published the extra-maxillary technique simultaneously (Aparicio C, Ouazzani W, Aparicio A, Fortes V, Muela R, Pascual A, Codesal M, Barluenga N, Manresa C, Franch M. Extrasinus zygomatic implants: three year experience from a new surgical approach for patients with pronounced buccal concavities in the edentulous maxilla. Clin Implant Dent Relat Res. 2010 Mar;12(1):55-61. doi: 10.1111/j.1708-8208.2008.00130.x. Epub 2008 Dec 3. PMID: 19076181. This article was accepted in 2006, published online in 2008, and print in 2010.) with Dr. Reginaldo Miglioranza (Migliorança et al. Exteriorização de fixações zigomáticas em relação ao seio maxilar: uma nova abordagem cirúrgica. Implant News, 3(1):30 2006).
This surgical technique opened the possibility of avoiding an intra-sinus path by placing the zygomatic implant more facially. This technique strongly reduces or even eliminates the risk of rhinosinusitis. However, a new long-term complication risk appeared: soft tissue dehiscence due to increased soft tissue tension due to the implant position.

The ZAGA Concept (2011-Today)
The ZAGA Concept was invented by Dr. Carlos Aparicio, and its first peer-reviewed publication was the ZAGA Book in 2012. Clinicians sometimes confuse the ZAGA Concept with the ZAGA classification.
The ZAGA classification is an anatomical evaluation of the concavity of the maxillary wall. Ranging from ZAGA 0 to ZAGA 4 allows an understanding of the shape of the maxillary wall and its future interaction with the zygomatic implant path.
The ZAGA Concept dives deeper into zygomatic implant rehabilitation by systematically defining the implant path based on anatomical, biomechanical, and prosthetic criteria. Indeed, while the in-depth explanation of the ZAGA Concept falls under the scope of a 3-day ZAGA Course, the objectives of the ZAGA concept are to provide a prosthetically-driven implant path while preventing long-term complications such as soft tissue dehiscence or rhinosinusitis.
To achieve this objective, the implant path is carefully studied and defined for each area: the zygomatic anchor zone, the antrostomy zone, and the zygomatic implant critical zone. Every surgery performed following the ZAGA Concept is patient-specific. Indeed, the initial incision, implant path, and closing of the soft tissue are personalized to each site and patient to reach a successful rehabilitation over time.
Since its creation, the ZAGA Concept has been widely published in peer-reviewed scientific journals. The original ZAGA Book was also completely updated, and a new edition was published in 2023.
A versatile portfolio of zygoma implants
The portfolio of ZAGA zygomatic implants is engineered from scratch to provide the right tools for the job. It is the first portfolio to provide two different designs to better adapt to each anatomical situation, following the same objectives. The ZAGA Round and ZAGA Flat implants have features that facilitate zygomatic implant success overall. Learn about each unique feature in the following section.
The Straumann zygoma portfolio is designed for the ZAGA Concept and also supports prior surgical techniques such as the Original, slot, or extra-maxillary techniques. However, one can reap all the benefits of the implant design only by using the ZAGA Concept. More details are in the upcoming section.
Features of the ZAGA zygomatic implants
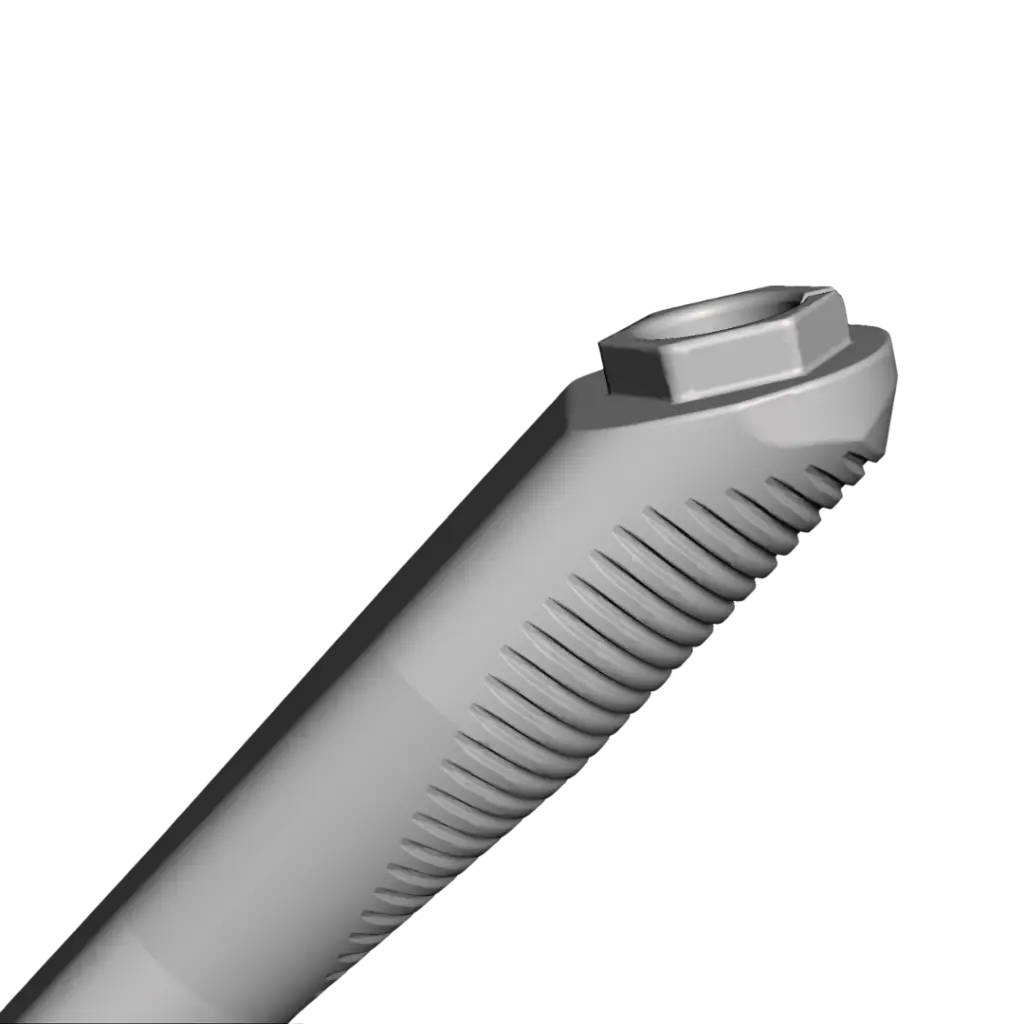
Angled platform
Tapered apex
Tapered regular dental implants have shown their benefits over time. Up to the design of the Straumann zygoma system, no zygomatic implant used the tapering effect for their stabilization in the zygoma bone. The ZAGA Round and ZAGA Flat have a tapered apex to maximize primary stability and ensure immediate loading capability.
Patients have increasing requirements for immediate procedures, and these features strongly support their needs. It is important to know that to make the most of the tapered apex, a ZAGA osteotomy should be used, preparing only the bed of the implant without the need for a second window or slot osteotomy.
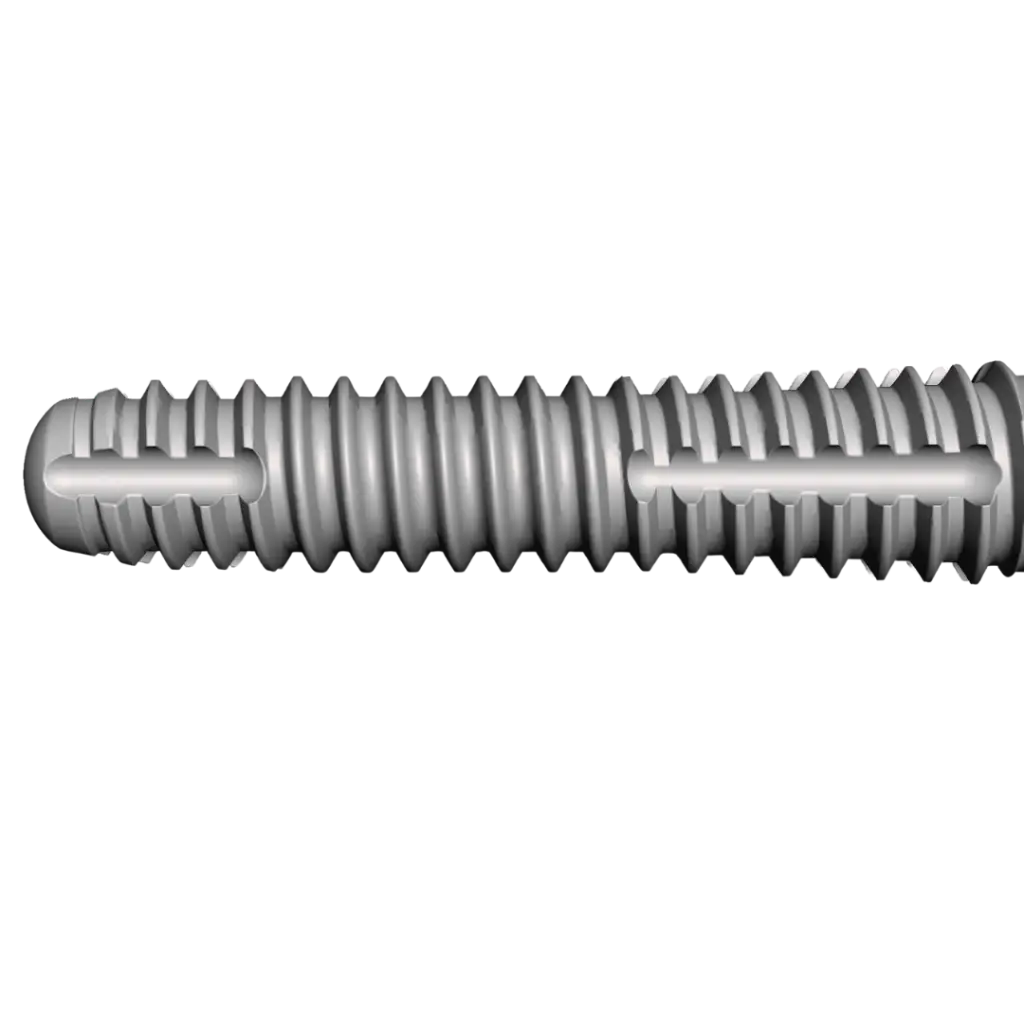
A flattened shaft
The ZAGA Flat zygomatic implant has an eye-catching feature: its flattened shaft. The objective of this characteristic is not to catch attention but, following the ZAGA Concept, better adapt to anatomies where an extra-maxillary path is chosen.
Indeed, soft tissue dehiscence arose as a long-term complication risk when using the extra-maxillary technique, despite removing the risk of rhinosinusitis almost completely. To support the challenges of an exteriorized approach, the ZAGA Flat implant shows a flattened profile facing the soft tissue facially to reduce the tension applied and, in turn, reduce the risk of soft tissue dehiscence in the long term.
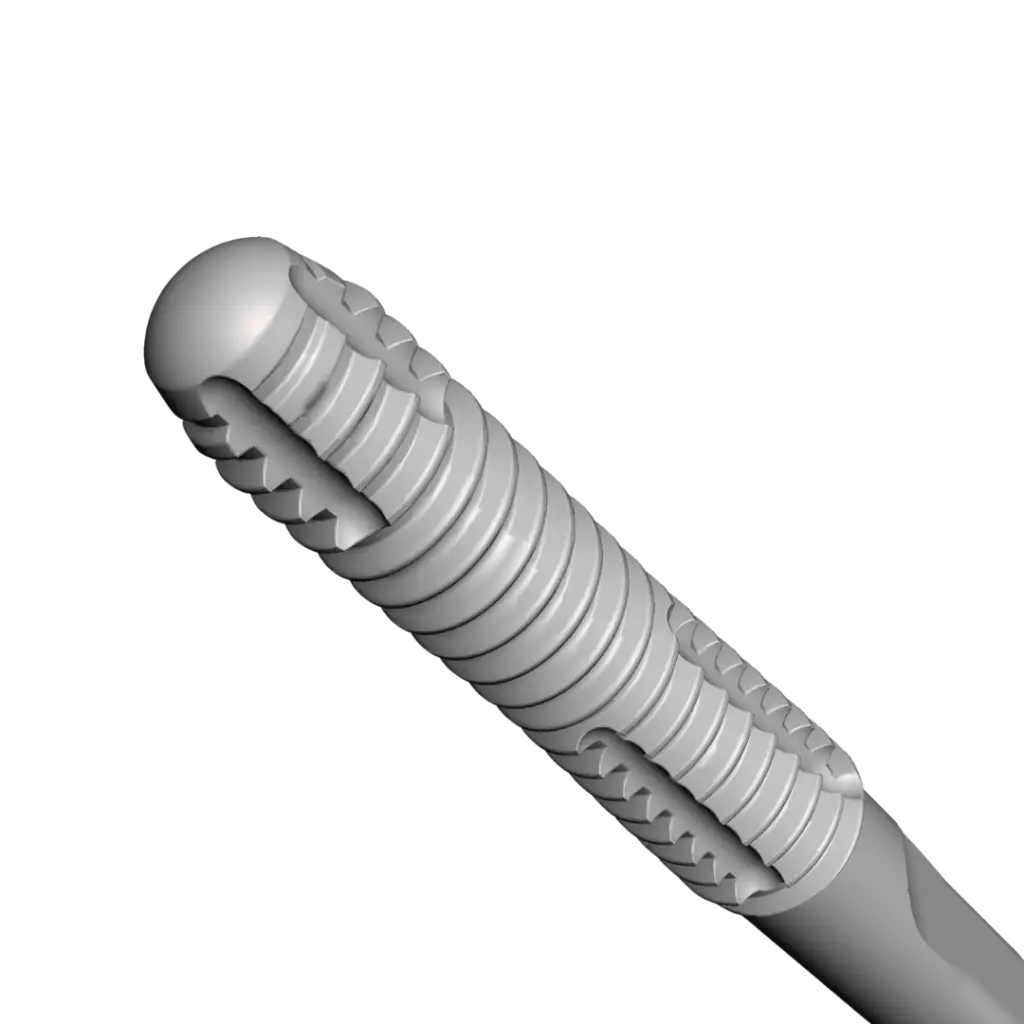
Rounded tip

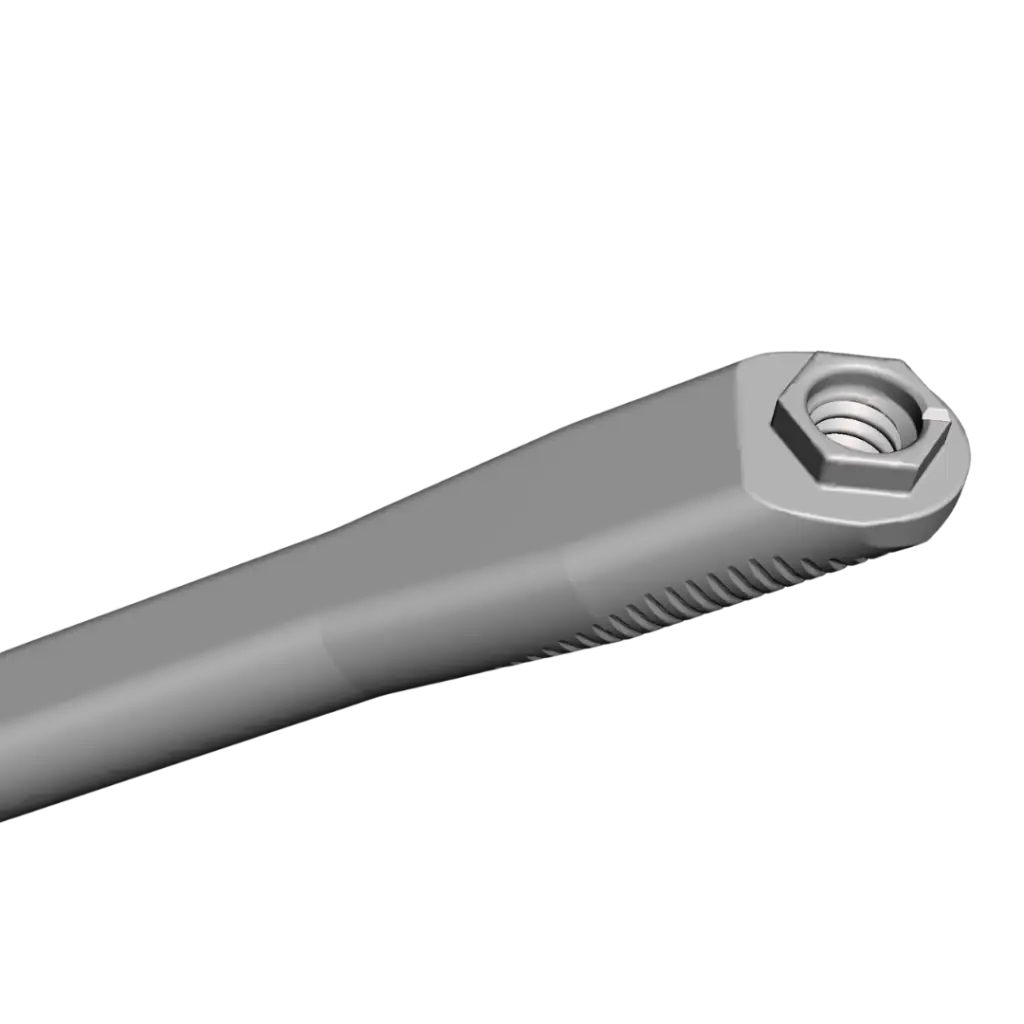
Implant Mount
Because not everything is in the design of an implant, the implant moun also plays a key role in making zygomatic surgeries more approachable and predictable. Past zygomatic implant designs included a large implant mount that interfered with its placement, especially in the anterior sector. The remains of the anterior alveolar bone could block the implant mount and prevent an adequate implant placement. This led to either the removal of the bone blockage or extremely complex placement.
The ZAGA zygomatic implants use an implant mount with the same external diameter as the implant body. Consequently, placing the implant is straightforward, and we can preserve the remains of the anterior alveolar bone. In the case of severe bone loss, protecting the remains of the bony structure is essential.

Reduced diameter
The ZAGA zygomatic implant system has a reduced diameter compared to classical manufacturers. This has numerous clinical benefits. First, it reduces the invasiveness of the procedure and post-surgical swelling. Second, the reduced diameter increases the angle between an anterior and posterior zygomatic implant in a quad situation.
This leads to a wider A-P spread and a better biomechanical situation for the long-term success of prosthetic rehabilitation. Despite their reduced diameter, the ZAGA implants do not show reduced fatigue resistance, thanks to the innovative pure Titanium they are composed of.
Scientific support of the ZAGA zygoma implants
1-year study
Clinical trials are valuable studies that help us understand the performance and viability of innovations. However, using inclusion and exclusion criteria for this type of study implies that the outcome does not reflect the actual clinical scenario. To evaluate the performance of the ZAGA zygomatic implant system, Dr. Carlos Aparicio led a group of experts in zygomatic implants (Dr. Waldemar D. Polido, Dr. James Chow, Dr. Rubén Davó & Dr. Bilal Al-Nawas ) to analyze 20 consecutive patients undergoing zygomatic implant rehabilitation in the network of certified ZAGA Centers.
The study concluded that both implant models are viable for their indication, within the study’s limits. Check the publication here: Aparicio, C. et al. Round and flat zygomatic implants: effectiveness after a 1-year follow-up non-interventional study. Int J Implant Dent 8, 13 (2022).

ZAGA Book
As mentioned, the way to make the most of the ZAGA implant designs is by following the ZAGA Concept from beginning to end. The new edition of the ZAGA Book by Dr. Carlos Aparicio and numerous collaborators presents the totality of the ZAGA Concept at the publishing date, including the planning protocol and procedures around soft tissue management to prevent long-term complications. This book highlights the ZAGA zygomatic implant portfolio and how to leverage their design to maximize the success of zygoma surgeries.

Specific training for zygomatic implants
ZAGA Centers organize 3-to 4-day courses focused on the ZAGA Concept. During the on-site or online courses, participants learn how to apply the ZAGA Concept in coordination with the ZAGA implants to provide excellent outcomes to their patients.