The ZAGA Concept: An Anatomy-Guided Approach to Zygomatic Implants
In short: The ZAGA Concept (Zygoma Anatomy-Guided Approach) is a clinical protocol developed by Dr. Carlos Aparicio for the rehabilitation of patients with severe atrophy of the upper jaw. It starts from an anatomical classification of the curvature of the maxillary wall (ZAGA Types 0 to 4). That classification defines the implant path on three sets of criteria – anatomical, biomechanical and prosthetic – and finally guides the choice between the two implant geometries designed by ZAGA and manufactured by Straumann: the ZAGA Round and the ZAGA Flat. ZAGA replaces the historical “one-size-fits-all” technique with a patient-specific protocol that reduces sinus complications, preserves soft tissue, and improves prosthetic outcomes – allowing in most cases a fixed full-arch restoration in less than 24 hours.

ZAGA stands for Zygoma Anatomy-Guided Approach. It is the clinical, surgical and prosthetic protocol developed by Dr. Carlos Aparicio (see Dr. Carlos Aparicio) for the rehabilitation of patients with severe atrophy of the upper jaw – the so-called “no-bone” patients – for whom conventional dental implants are not a viable solution and bone grafting would be complex, prolonged or unwanted.
Unlike earlier zygomatic implant techniques – which forced every patient into the same intra-sinus trajectory – the ZAGA Concept begins with each patient`s anatomy and adapts every subsequent decision to it: the implant path, the osteotomy, the soft-tissue management, the implant geometry, and the prosthetic emergence. It is an anatomy-centred model, not a technique-centred model.
First described in the peer-reviewed publication “A proposed classification for zygomatic implant patient based on the zygoma anatomy guided approach (ZAGA)” (Aparicio et al., Clin Implant Dent Relat Res 2011), the concept has since evolved into a complete protocol covering anatomical classification, surgical execution, implant design and long-term prosthetic outcomes (see ZAGA Science).
From "Surgical Recipe" to Anatomy-Guided Protocol
For more than two decades, zygomatic implant placement followed a standardised intra-sinus trajectory. While effective in many patients, the rigid “one technique fits all” approach was associated with a recurring pattern of complications:
- post-operative sinusitis and chronic sinus inflammation
- oro-antral communications
- buccal soft-tissue dehiscence and implant exposure
- palatally emerging, bulky prostheses limiting hygiene, phonetics and aesthetics
The ZAGA Concept introduced a paradigm shift: every surgical and prosthetic decision is derived from the patient`s residual anatomy. As Dr. Aparicio summarises it, “ZAGA is more than a method – it is a philosophy”, with patient well-being, long-term success and the prevention of complications as its core principles.
The ZAGA Anatomical Classification of the Maxillary Wall
The starting point of the ZAGA Concept is an objective, reproducible classification of the concavity (curvature) of the maxillary wall at the implant site. Using CBCT imaging, the surgeon classifies each implant site as ZAGA Type 0, 1, 2, 3 or 4.
In the original Aparicio cohort, the prevalence of each type was 15%, 49%, 20.5%, 9% and 6.5%, respectively (Aparicio 2011), demonstrating that most sites fall between Type 1 and Type 2 – and that anatomical variability is the rule, not the exception.
A high-definition printed 3D model is highly recommended to deeply understand the anatomy of the region.
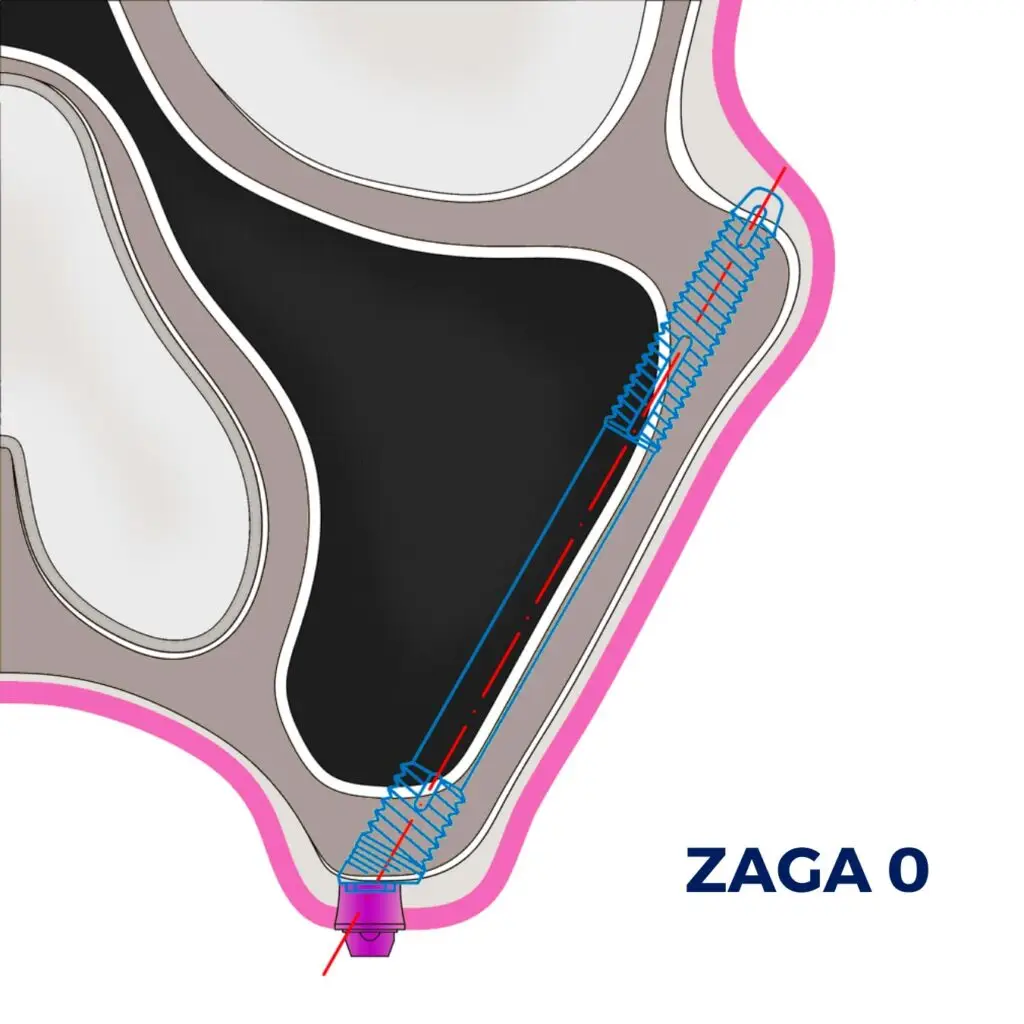
ZAGA Type 0
A convex lateral maxillary wall with sufficient residual alveolar and lateral bone. A fully intra-sinus trajectory is feasible, and the prosthetic emergence is favourable at the crest.
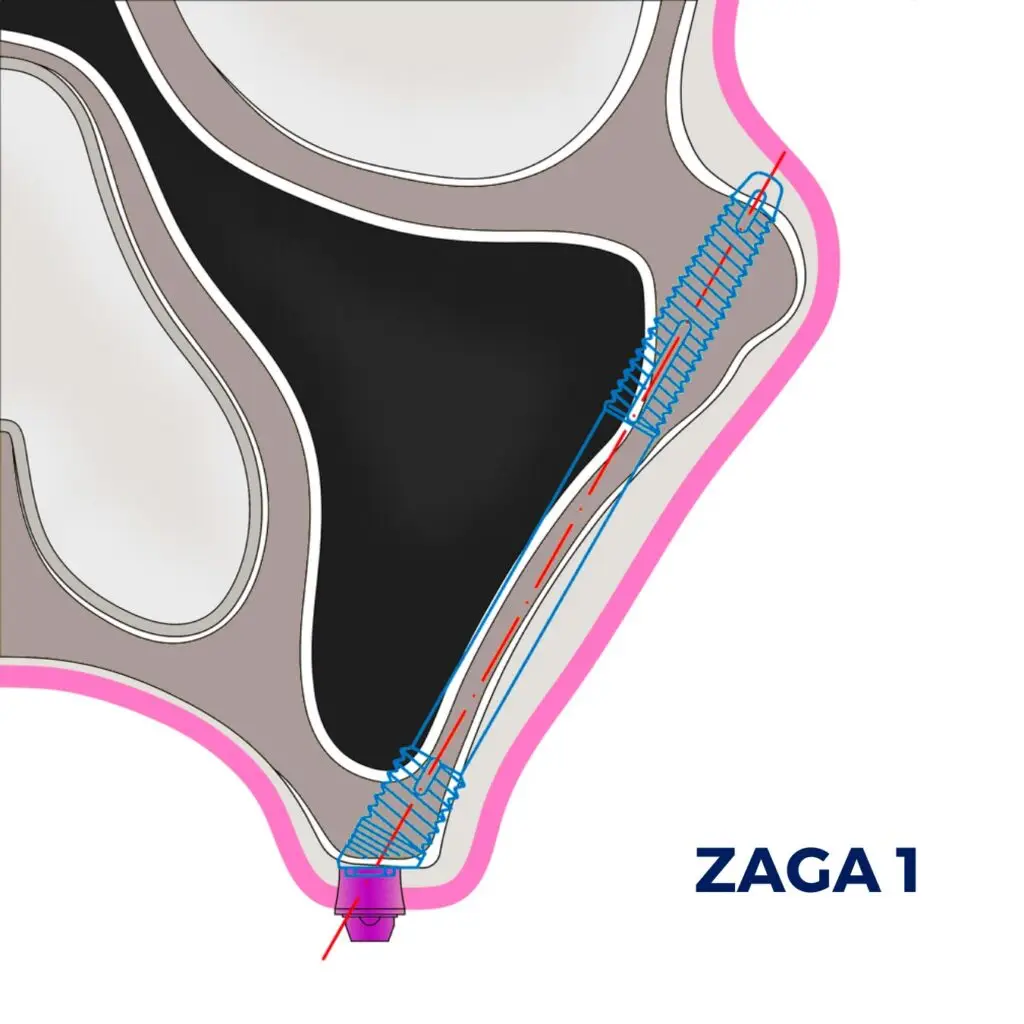
ZAGA Type 1
A slightly concave wall with adequate bone preserved at the alveolar crest. The implant path remains predominantly intra-sinus, with limited contact between the implant body and the lateral wall.
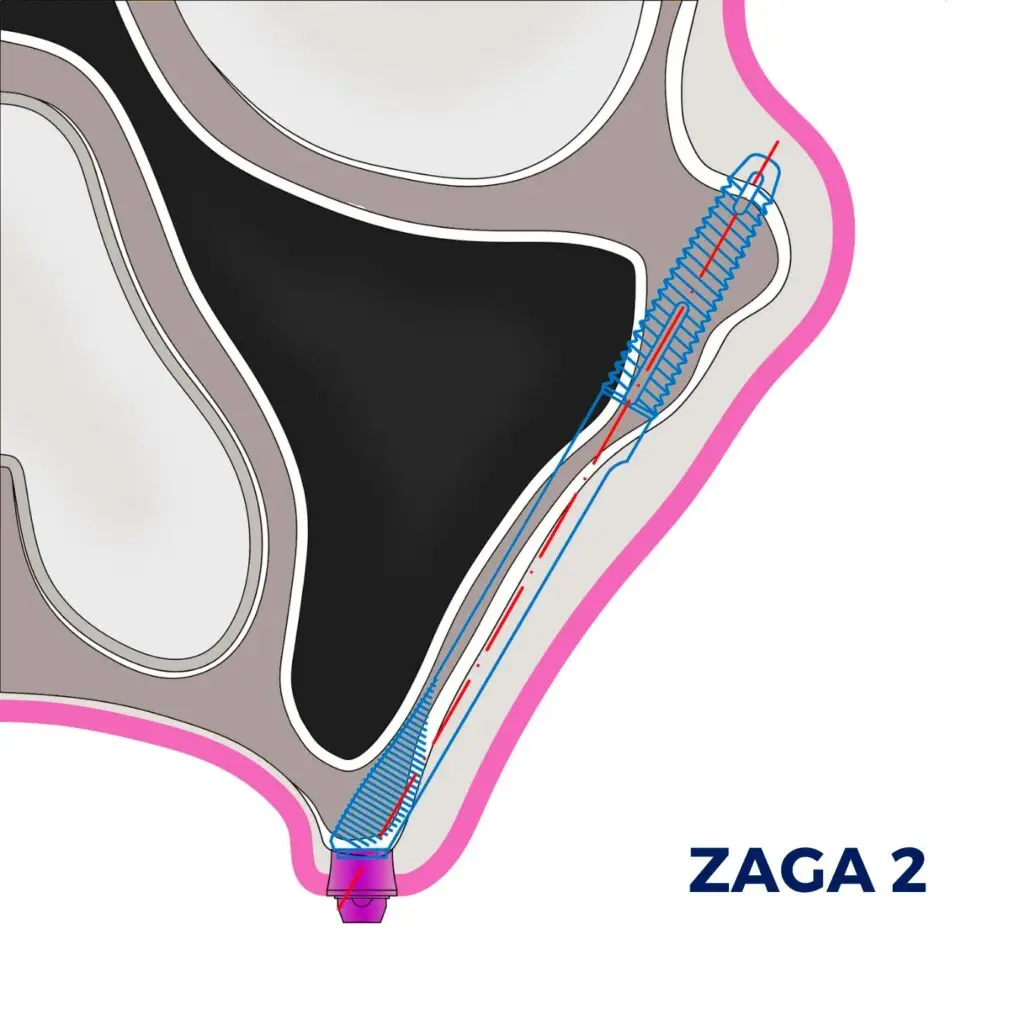
ZAGA Type 2
A pronounced concavity of the maxillary wall, with bone still preserved at the crest. The path is typically hybrid: the implant begins at the alveolar crest, exits the lateral wall, runs extra-sinus, and re-enters the bone to anchor in the zygoma.
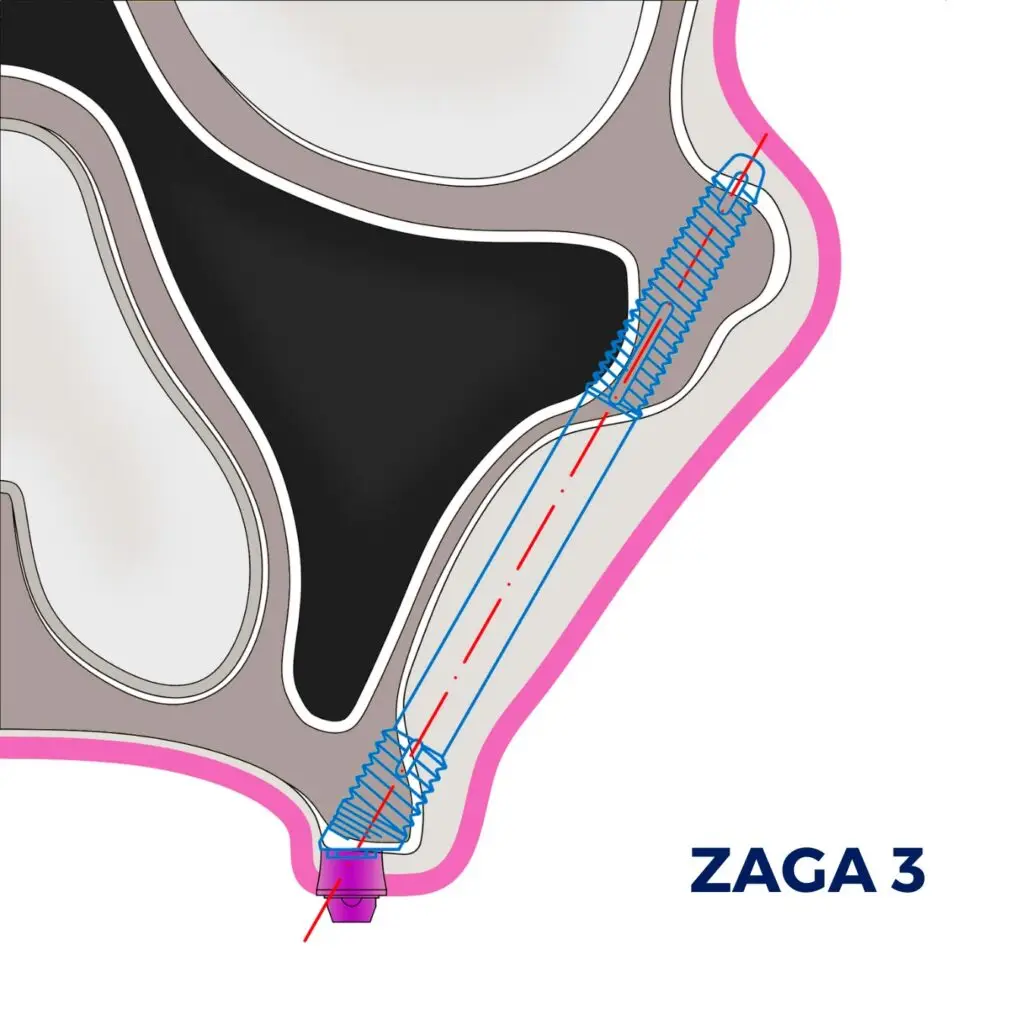
ZAGA Type 3
A severely concave wall combined with a reduced anterior-posterior dimension of the maxilla. The trajectory is predominantly extra-sinus.
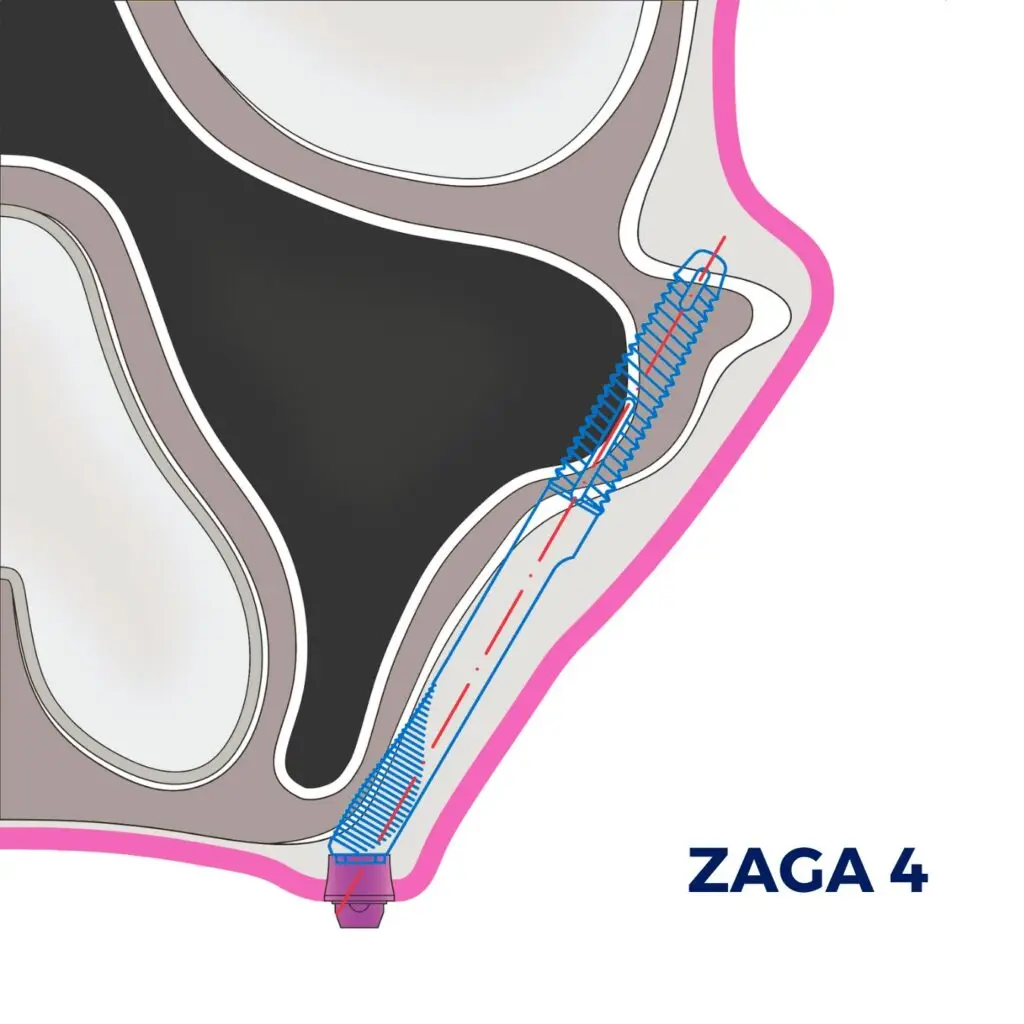
ZAGA Type 4
Minimal residual alveolar bone with a severely concave wall. The implant path is fully extra-sinus and anchored exclusively in the zygomatic bone.
From Anatomy to Implant Path: Anatomical, Biomechanical and Prosthetic Criteria
The classification is not an end in itself. It defines the implant path through three complementary lenses:
- Anatomical criteria – the shape and thickness of the maxillary wall, the sinus anatomy and status, the residual alveolar bone volume and shape, and the soft-tissue (gingival) conditions at the planned emergence.
- Biomechanical criteria – engagement of both the alveolar crest and the body of the zygoma, primary stability for immediate loading, and long-term distribution of occlusal forces along the zygomatic buttress.
- Prosthetic criteria – emergence of the implant platform as close to the alveolar crest as possible, allowing a non-bulky, hygienic, phonetically comfortable and aesthetic full-arch restoration.
The chosen path may therefore be intra-sinus, extra-sinus, or hybrid – but in every case it is the consequence of the anatomical classification, not a default. The ZAGA Concept also recommends, whenever the residual anatomy allows it, a tunnel-type osteotomy that preserves both the alveolar crest and the lateral wall.
Learn the ZAGA Concept Now
Online course
Enroll now and start learning from anywhere, immediately! Learn at your own pace by going through the 11 modules and quizzes!
Cadaver course
Upon completion, you will receive a valid 15 CE certificate for 15 hours of learning. You will have to successfully complete all Quizzes to receive it!
Live Surgery Training
The completion of the Online ZAGA Course opens the doors to the ZAGA Certification to become the exclusive ZAGA Center in your area.
Choosing the Right Implant: ZAGA Round and ZAGA Flat by Straumann
Once the implant path has been defined, the ZAGA Concept guides the selection of the implant geometry itself. The two implants of the Straumann zygomatic portfolio – designed by ZAGA and launched commercially by Straumann in October 2020 – are co-engineered for exactly this purpose. The full technical specification of each implant is detailed on the dedicated page The Straumann ZAGA Zygomatic Implants.


ZAGA Round
Circular cross-section along the entire body. Optimised for tunnel-type osteotomies and intra-sinus paths, typically indicated in ZAGA Types 0 and 1 and selected hybrid Type 2 cases. The threaded neck helps to achieve and maintain osseointegration at the alveolar crest, while the tapered apex secures primary stability in the zygoma.
ZAGA Flat
Flattened mid-portion and coronal section. Specifically engineered for extra-maxillary trajectories – where the implant body runs along or outside the lateral wall – the flat shaft reduces soft-tissue tension and minimises the risk of vestibular dehiscence. Primarily indicated in ZAGA Types 2 and 4.
Both implants share a 55-degree angled platform, a tapered rough apex for primary stability, a reduced 3.4 mm apex diameter optimised for fatigue strength, and a turned (machined) coronal portion designed to discourage bacterial adhesion at soft-tissue level.
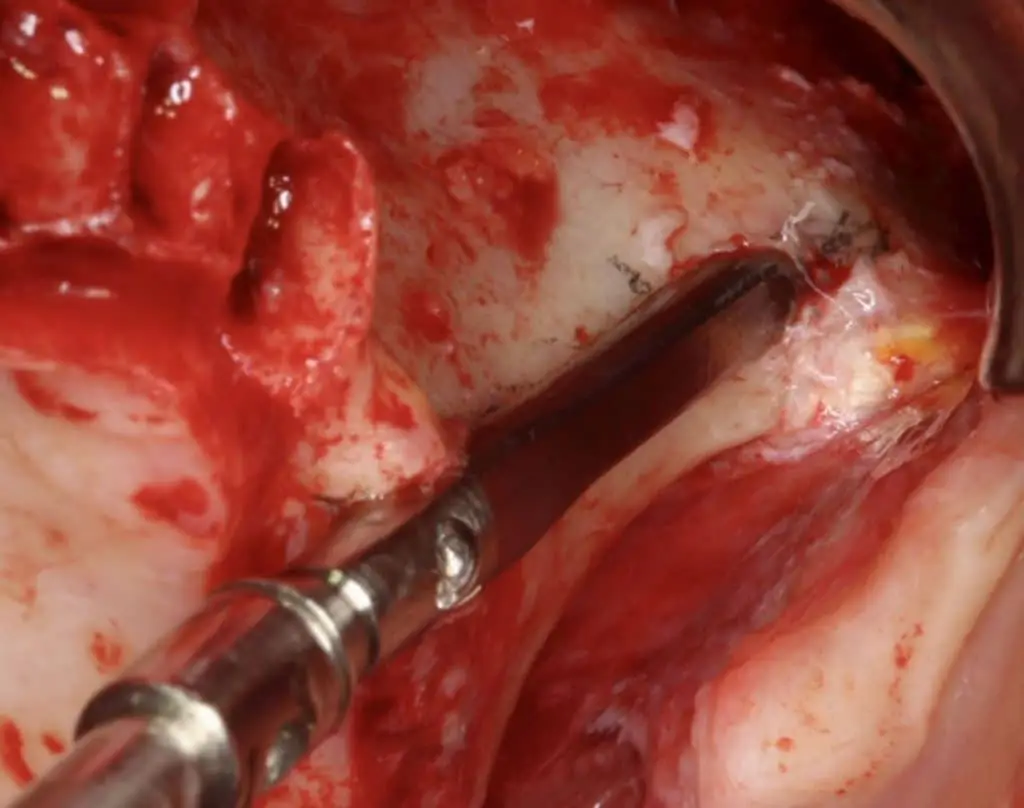
The ZAGA Minimally Invasive Osteotomy
The osteotomy is individualised in the same way as the implant choice. The ZAGA Minimally Invasive Osteotomy preserves both the alveolar crest and the residual maxillary wall, reduces sinus invasion whenever possible, and protects the soft-tissue envelope – or even allows it to be augmented during healing. Compared with classical lateral antrostomies, it limits unnecessary bone removal, reduces the size of any oral-antral communication, and shortens the post-operative recovery.
Clinical Outcomes: The ORIS Success Criteria
Long-term success in zygomatic implantology cannot be reduced to a single “implant survival” rate. The ZAGA scientific work introduced the ORIS criteria, four parameters that together define a successful long-term outcome:
O
Offset: prosthetic emergence position (palatal vs. crestal) – the closer to the alveolar crest, the better the prosthetic and hygienic outcome.
R
Rhinosinus status: sinus health assessed on clinical examination and radiographic imaging.
I
Implant soft tissue: integrity of the peri-implant mucosa, absence of dehiscence and exposure of the implant body.
S
Stability: clinical absence of mobility on standardised testing.
A 10-year follow-up study (Aparicio et al., J Clin Med 2023) confirmed superior sinus status and prosthetic offset outcomes for ZAGA-treated patients compared with historical non-anatomy-guided cohorts. The complete bibliography is available at ZAGA Science.

Who Benefits from the ZAGA Concept?
The ZAGA Concept is indicated for adult patients presenting with:
- severe atrophy of the upper jaw or “no-bone” maxillae
- complete edentulism without sufficient bone for conventional implants
- cases in which bone grafting (sinus lift, iliac crest graft) is undesirable, contraindicated, or has failed
- rescue of failed conventional or zygomatic implants
- patients seeking a fixed full-arch restoration in less than 24 hours from surgery
Patients researching their treatment options can find a step-by-step, patient-friendly explanation of the journey on our patient portal Smile24h, and locate a certified surgeon through the international network.
Scientific Evidence Behind the ZAGA Concept
The ZAGA Concept is supported by more than a decade of peer-reviewed scientific publications, including:
- Aparicio C, Manresa C, Francisco K, et al. A proposed classification for zygomatic implant patient based on the zygoma anatomy guided approach (ZAGA). Clin Implant Dent Relat Res 2011.
- Aparicio C (ed.). Zygomatic Implants: The Anatomy-Guided Approach. Quintessence Publishing, 2012.
- Aparicio C, Polido WD, Chow J, et al. Round and flat zygomatic implants: effectiveness after a 1-year follow-up non-interventional study. Int J Implant Dent 2022.
- Aparicio C, Polido WD, et al. Round and flat zygomatic implants: effectiveness after a 3-year follow-up non-interventional study. Int J Implant Dent 2024.
- Aparicio C, et al. The Zygomatic Anatomy-Guided Approach, Zygomatic Orbital Floor Classification, and ORIS Criteria – A 10-Year Follow-Up. J Clin Med 2023.
A complete and continually updated bibliography is maintained at ZAGA Science, and the full protocol is detailed in the Advanced Zygomatic Implant Book.
Becoming a ZAGA-Certified Clinician
The ZAGA Concept is taught exclusively through the ZAGA Course programme, which combines the ZAGA Zygomatic Implant Online Course, live surgery courses, cadaver training, and one-to-one ZAGA Mentoring. Certified clinicians join the ZAGA Network and may apply for ZAGA Center certification.

Frequently Asked Questions about the ZAGA Concept
The ZAGA Concept was developed by Dr. Carlos Aparicio (MD, DDS, MSc, MSc, DLT, PhD), first published in 2011 and continuously refined since. He is the Scientific Director of the ZAGA Centers network - see Dr. Carlos Aparicio [/zaga-network/dr-carlos-aparicio/].
Both. ZAGA is, first, an anatomy-guided clinical protocol. Second, it is a portfolio of implants - the ZAGA Round and the ZAGA Flat - designed by ZAGA and manufactured by Straumann to support that protocol.
The maxillary wall is classified (ZAGA Type 0 to 4) on CBCT. That classification defines the implant path; the path determines whether a ZAGA Round (intra-sinus / tunnel-type) or a ZAGA Flat (extra-maxillary, Types 2 and 4) implant is indicated.
In most cases, a fixed provisional full-arch prosthesis is delivered in less than 24 hours after surgery. Final eligibility is decided by the treating surgeon based on the primary stability achieved.
The international list of certified clinicians and ZAGA Centers is published at the ZAGA Network [/zaga-network/]. A referral form is available at Refer me to a certified expert [/zygomatic-implants-referral-to-certified-experts/].
By adapting the implant path to the patient`s anatomy instead of forcing a standardised intra-sinus trajectory, the ZAGA Concept reduces sinus invasion, preserves soft tissue, and improves the position of the prosthetic platform - the three drivers of the historical complication profile.